Tibial stress fractures- does running form matter?
What Was the Study About?
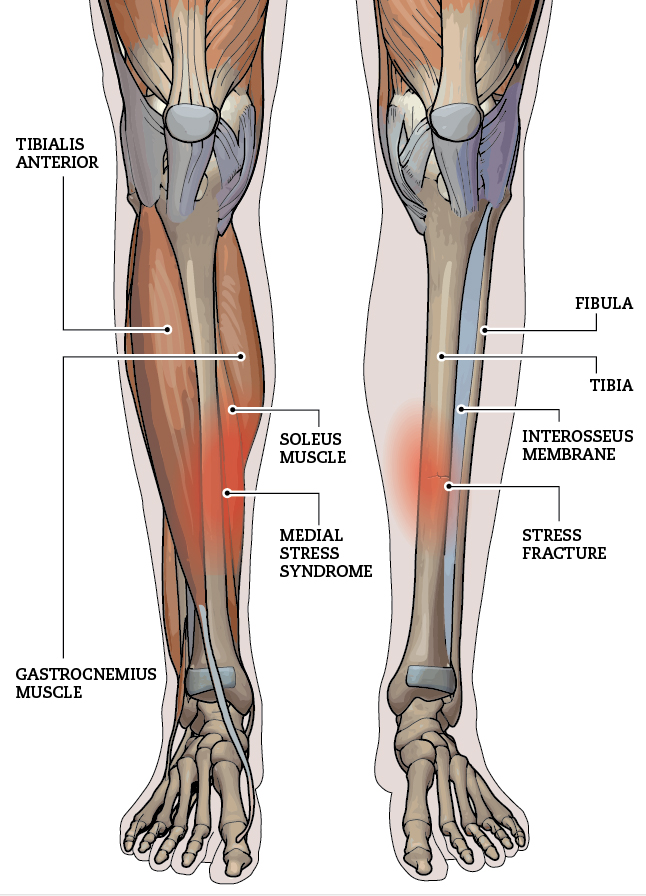
Tibial stress fractures (TSFs) are common overuse injuries in runners. They happen when repeated force on the shinbone causes tiny cracks that outpace the body’s ability to repair them. Many clinicians and coaches think that the way someone runs – their biomechanics – might influence who gets these injuries. This 2023 review study set out to find out whether runners with TSFs really move differently from runners without them.
How Did They Study It?
The authors searched major research databases for studies that compared running mechanics between injured runners and healthy controls. They found 359 possible papers, but only 14 met strict criteria for analysis. Most of these studies were retrospective (looking back at runners after injury) and had small sample sizes- so as always, more research that prospective and more controlled would be nice!
What Did They Find?
When all the data were combined:
- There were no significant differences in ground reaction forces between runners with TSFs and uninjured runners. In other words, impact and braking forces were similar in both groups.
Some individual studies did find differences in variables like tibial stress, tibial acceleration, rearfoot motion, or hip movement, but these findings were not consistent across studies.
What Does This Mean?
Based on the best available evidence:
- We can’t confidently say that runners with tibial stress fractures have a distinct running biomechanics profile.
- Current studies are too small and too varied to draw strong conclusions.
- Larger, better‑designed research is needed to clarify whether specific movement patterns truly increase the risk of TSFs.
- In the meantime- stick with the things we KNOW related to printing stress fractures:
- Adequate caloric intake
- Vitamin D supplementation
- Adequate calcium intake
- Strength work
- Being smart with your training load- building slowly, taking recovery days and weeks strategically
If you have any questions about pain you’ve been feeling- feel free to contact our Waterloo based chiropractors, physiotherapists or book online HERE.