Surgical vs. Non-Surgical Treatment for Partial Rotator Cuff Tears
By: Dr. Sean Delanghe BSc (Hons), DC
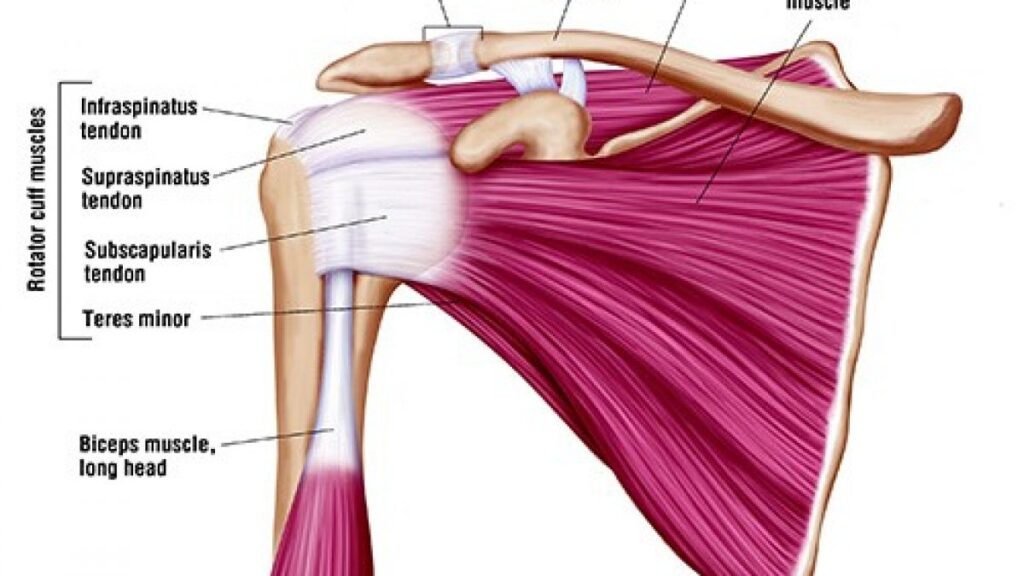
The rotator cuff is a group of four muscles that originate from the shoulder blade (scapula) and attach to the humerus through their tendons. The primary function of the rotator cuff is to provide dynamic stability to the shoulder joint by keeping the head of the humerus centered within the glenoid socket during movement. These muscles also contribute to shoulder movements, including lifting the arm and performing internal and external rotation.
Partial-thickness rotator cuff tears (PT-RCTs) are a common cause of shoulder pain and reduced function. These injuries occur when the rotator cuff tendon is damaged but not completely torn. Both surgical and non-surgical treatments are used to manage these injuries; however, there remains uncertainty regarding which treatment approach provides the best outcomes.
The purpose of this 2026 study was to compare surgical and non-surgical treatments for partial rotator cuff tears and determine whether one approach provides superior clinical outcomes.
Results
This study was a systematic review and meta-analysis, meaning the researchers collected and combined results from multiple previous studies- this is as high of quality of evidence that you can get!
Included Studies
- 9,894 studies were initially screened.
- 33 studies met the inclusion criteria.
- A total of 1,818 patients were included in the analysis.
Surgery Compared With Non-Surgical Treatment
Results:
- Surgical treatment groups demonstrated statistically better shoulder function scores compared with non-surgical treatment groups- but these differnce wer extremely small!
- Despite these statistical improvements, the differences did not exceed the minimal clinically important difference.
- This means that although surgery produced better scores on testing, the average improvement may not be large enough for patients to notice a meaningful difference in daily life.
Comparison of Different Surgical Techniques
The study also compared different surgical approaches.
Repair involves surgically reattaching or restoring the torn tendon back to the bone, while debridement involves removing damaged or frayed tendon tissue without repairing the remaining tendon
Results:
- No statistically significant difference was found between tendon repair and debridement.
- Neither surgical approach demonstrated clear superiority.
Tear Completion Repair vs. Transtendon Repair
Tear completion repair finishes the partial tear into a full tear before repairing it, while transtendon repair preserves the remaining intact tendon by repairing the tear without fully cutting through it.
Results:
- No significant differences were found between the two repair techniques.
- Both techniques improved patient outcomes, but neither was shown to be more effective.
Practical Applications
The findings of this systematic review suggest that surgery can improve shoulder function in patients with partial rotator cuff tears. However, the advantage of surgery compared with non-surgical treatment appears to be relatively small and may not represent a clinically meaningful difference for many patients.
On top of that, surgery comes with it’s own risks and delay in recovery and simply deso not exist if you chose a conserative plan (relative rest, progressive loading with a structure physio plane etc).
The authors suggest that treatment decisions should be individualized. Factors such as symptom severity, functional limitations, patient goals, and response to rehabilitation should be considered when deciding whether surgery is appropriate.
If you have any questions about your rotator cuff injury, feel free to reach out to any of our Waterloo based chiropractors, physiotherpists or RMTs HERE.