Stress fractures 101!
By. Dr Sean Delanghe BSc (Hons), DC
There’s nothing worse than hearing you have a stress fracture as a runner (maybe)! This 2024 review of systematic review will help to arm you with the information you need to avoid them and catch them early!

What This Study Is About
Stress fractures are overuse injuries that develop when repeated mechanical loading exceeds the bone’s ability to recover. The paper explores how frequently these injuries occur, where they are most likely to happen, what contributes to their development, and how they are best diagnosed and treated.
How the Research Was Done
The authors reviewed evidence from major databases – primarily systematic reviews. Around 90 studies were initially identified, with approximately 57 included in the final analysis. This is the best of the best!
Where Stress Fractures Happen Most
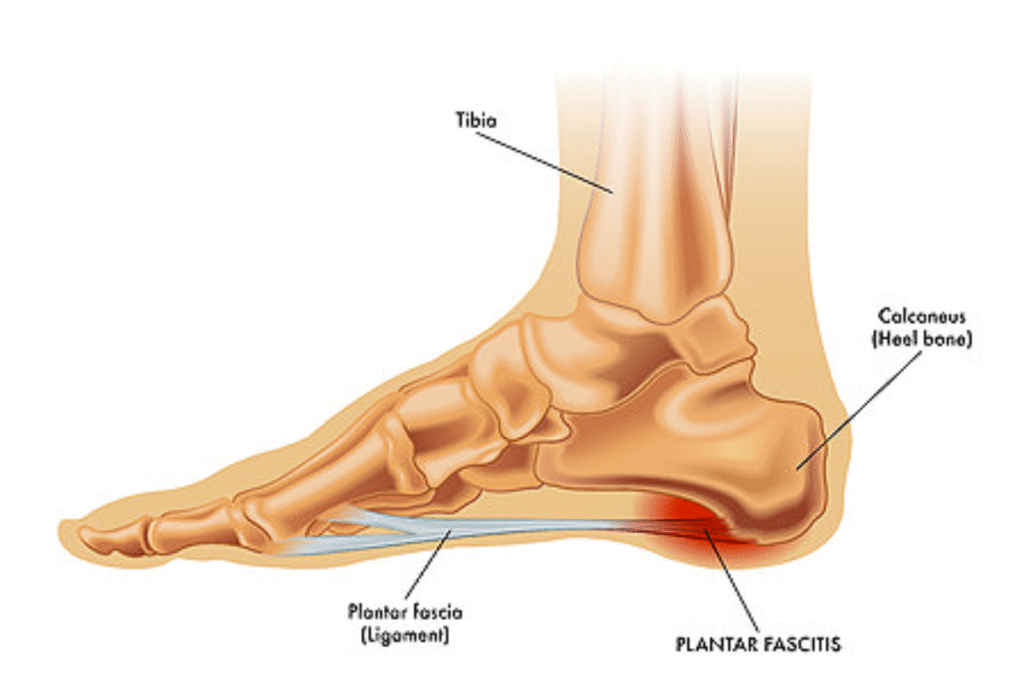
Stress fractures occur predominantly in the lower extremities due to repetitive loading during running. In long-distance runners, the tibia is the most commonly affected bone, followed by the metatarsals. In contrast, sprinters tend to experience more stress fractures in the toe bones, likely due to the higher forces and forefoot loading associated with sprinting mechanics.
Why Stress Fractures Develop
Stress fractures are multifactorial and typically result from a combination of biological, nutritional, mechanical, and psychological factors.
Key factors include:
- female sex
- reduced bone density
- nutritional factors such as low energy availability and deficiencies in calcium or vitamin
- Training-related issues, particularly rapid increases in workload
- In addition, psychological factors like high stress levels, perfectionism, and fear of failure may indirectly increase injury risk by influencing training behaviours and recovery.
How They Are Diagnosed
Diagnosis begins with a detailed clinical history and physical examination, but imaging is often required for confirmation.
- MRI is considered the most sensitive and preferred method for detecting stress fractures, especially in the early stages.
- X-rays are commonly used but may not detect early bone stress injuries, which can delay diagnosis if relied upon alone.
- Bone scans are the fastest and most sensitive option for most of us in Canada.
What Treatment Looks Like
Treatment primarily involves reducing or temporarily stopping the activity that caused the injury, allowing the bone time to heal. A gradual return to running is introduced once symptoms improve. Importantly, treatment should also address the underlying factors that contributed to the injury- see above!
How to Reduce Your Risk
Preventing stress fractures requires a proactive approach that includes maintaining adequate nutrition and energy availability, progressing training loads gradually, and addressing any biomechanical inefficiencies. Screening for conditions such as RED-S or the Female Athlete Triad may also be important in certain populations. Psychological stress should not be overlooked, as it can influence both training habits and recovery- are you doing the right thing for your training, or are you responding to anxiety that is telling you to illogically ramp up?
Practical applications:
- Most stress fractures occur in the lower extremities
- Tibia is the most common site in long-distance runners
- Metatarsals are the second most common
- Sprinters more commonly experience stress fractures in the toes
- Risk factors include biological, nutritional, mechanical, and psychological components
- MRI is the most sensitive diagnostic tool, bone scan is probably our best choice in Canada
- Treatment focuses on rest, gradual return, and addressing underlying causes
- Prevention requires proper training progression, nutrition, and overall load management
- Managing anxiety related to training and racing is a huge factor for most competitive runners!
If you have any questions about any of your injures for our Waterloo based chiropractors, physios or RMTs- feel free to contact us or book online HERE.





 munology notes yet again to relearn what I already know (it’s always fun picturing the T-cells destroying the bad stuff). Times like these also motivate me to relearn other things, like how nothing gets rid of a cold other than some basics including: sufficient rest, fluids, stress management and a good diet.
munology notes yet again to relearn what I already know (it’s always fun picturing the T-cells destroying the bad stuff). Times like these also motivate me to relearn other things, like how nothing gets rid of a cold other than some basics including: sufficient rest, fluids, stress management and a good diet.