Welcome back to my series on strength training for endurance athletes. Last article took a look at the role (or lack there of) of strength training and our ability to consume oxygen.
That being said, we still know that strength training does have a positive impact on performance in endurance athletes. The caveat: it has to be the right type of athlete, with the right type of deficiency conducting it at the right time in training.
So how do we decide how and when to implement strength training? Learning the science of how it impacts us helps to guide these decisions in the best possible way. This series most definitely is not a clear-cut, quick-fix answer, nor is it remotely all inclusive. The more you learn, the more you will realize there is to learn! Heck, I went to school for 8 years after high school in human-physiology related fields followed by 10 years in working and coaching in the field- and I definitely still feel like the more I learn, the more confusing it can become at times!
That being said, the more information you arm yourself with, the more you will be able to start to tell the difference between pseudoscientific advice and real, efficient and effective performance-boosting advice. Our next step toward this direction: How it impacts our exercise economy…
It’s been a while! Life has been insanely busy the past couple months. You might have noticed on my social media feeds that I have moved my physiotherapy practice to join forces with Delanghe Chiropractic & Health/Health & Performance. Pumped for what this opportunity will bring!
So what’s on the agenda today? In honour of a few patients I have seen recently for a variety of running related injuries, we will be addressing the question: do injured runners run differently?
I will be drawing from an article by Christopher Bramah published in 2018 that looks at this very issue. He compared healthy runners (no reported injury in over 18 months) to injured runners to see if there were any run gait characteristics that were predictive of current injury. He specifically looked at the four most commonly cited soft tissue injuries in the running population: Patellofemoral Pain Syndrome, Iliotibial Band Syndrome, Medial Tibial Stress Syndrome, Achilles Tendinitis.
(Let’s just acknowledge the fact that I haven’t used Microsoft Paint in possibly a decade. How is it still a thing?)
You might not have heard of these conditions before, but you have probably experienced them. Here is a quick breakdown of what each of these injuries involve in the simplest of terms:
Patellofemoral Pain Syndrome (PFPS): pain around the patella, aka the knee cap at the front of the knee
Iliotibial Band Syndrome (ITBS): pain at the outside of the knee
Medial Tibial Stress Syndrome (MTSS): AKA Shin Splints (the bane of my existence for many years), pain around the inner part of the bottom 1/3 of the shin.
Achilles Tendinitis (AT): pain at the Achilles tendon.
I have to say, it’s always pretty neat when the findings of a study are similar to what you experience clinically. After analyzing the running biomechanics of the injured and non-injured study participants, Bramah’s team found that the injured runners presented with:
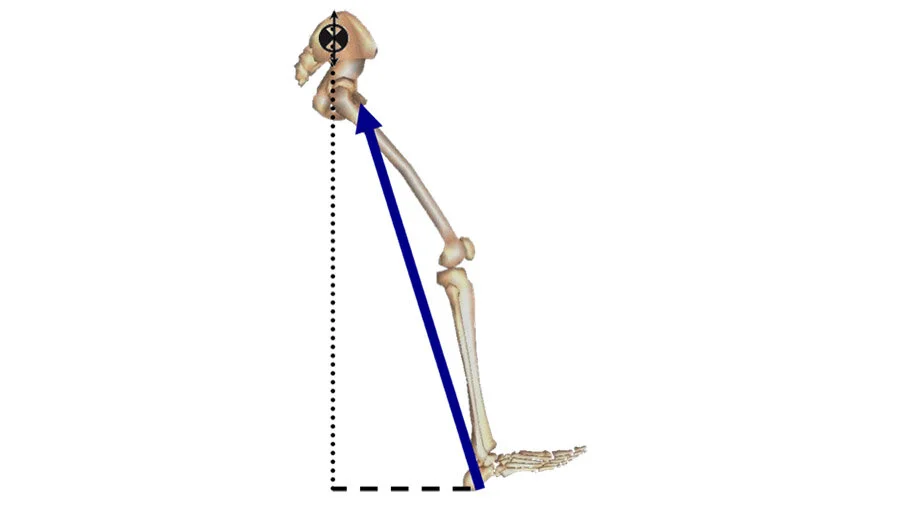
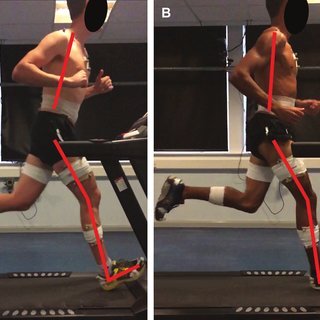
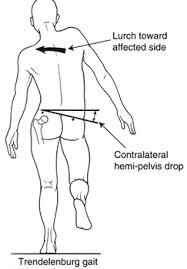
A straighter knee and ankle dorsiflexion (toes pulled up to the shin) when landing. This is essentially what we would call overstriding/overreaching while running – your foot is way out in front of your center of mass when you first hit the ground.Increased forward trunk lean. This can be caused by low back and gluteus maximus weakness/fatigue. We need to strike a balance of leaning forward too much and sitting back like you’re in a La-Z-Boy. Photo is from the Bramah et al. 2018 article.A significant drop in the opposite hip to the one they are standing on, also known as a Trendelenburg. This can be a sign of weakness of the hip stabilizing muscles on the leg they are standing on because they cannot keep the pelvis level. Note that the hip drop was found to be the most accurate at predicting if the runner was injured.
These are pretty important to note because they can actually exacerbate your injury by adding stress to the already injured tissues. Talk about adding insult to injury!
I do have to acknowledge that not every runner is the same. There are some runners that are FAST, have a wicked hip drop, and are totally functional. But as a physiotherapist, it is good for me to keep in mind that these running traits are often present with an injured runner.
What are the implications?
If you are a runner dealing with any type of injury, come in and get assessed. The weather is warming up and nothing is more of a bummer than not being able to get out there and enjoy it.
I do not believe that all runners should run the same way. However, I am not opposed to tweaking your run form to help iron out some of these movements patterns. Gait assessments are a great way to get a second set of eyes on your run form and see if there is anything we can adjust with cueing.
On top of running tips, I always give some homework to help you move better. I typically assign a short list of exercises that are targeted to your concerns – all business, no filler.
Don’t let nagging injuries keep you on the couch! Let’s work together to get you back out there! Click here to book now
In both kinesiology and physiotherapy school, we were taught anatomy. The sheer volume of knowledge was overwhelming. Where does each muscle attach? What nerve controls which muscle? It felt like we were learning everything there was to know about the body. That was incredibly naive of me, as research has plowed on and has shown just how complex our movement systems are.
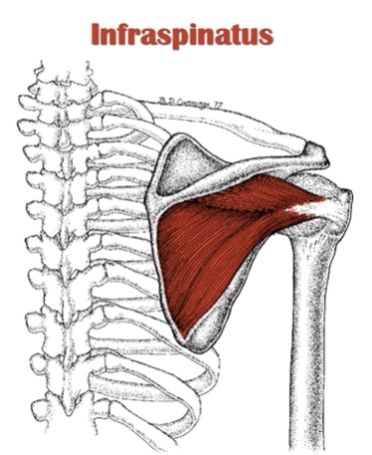
This post will take a closer look at the infraspinatus, one of your four rotator cuff (RC) muscles. Located just under the boney ridge of your shoulder blade, it is commonly injured, especially in overhead athletes (throwers, climbers, etc).
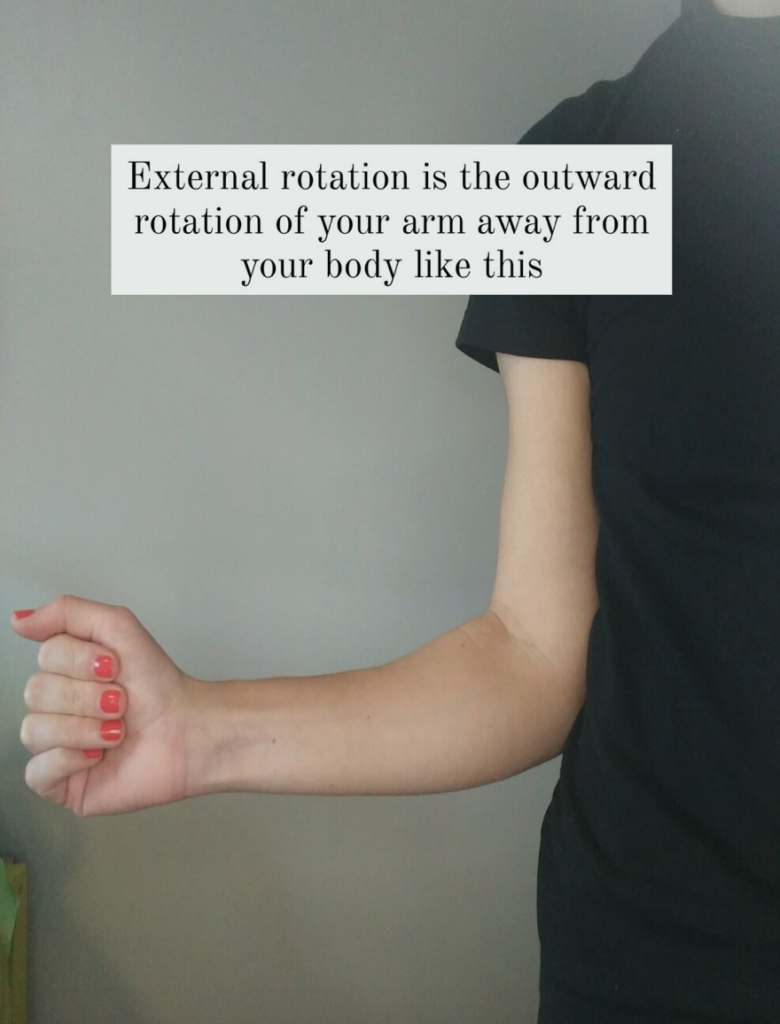
When I learned about the infraspinatus, we were told that it was a muscle that externally rotates, or turns your arm outward (see below for a picture showing that position) and that it is controlled by your suprascapular nerve. But within the last 20 years or so, researchers have found that the infraspinatus has three distinct regions, each innervated by its own mini branch of the suprascapular nerve; the superior, middle, and inferior infraspinatus subregions.
Why does this matter? Well, turns out that the subdivisions serve slightly different purposes, kind of like how your municipality functions within the province. The province of Ontario has an overarching goals, but Waterloo Region will function in a different way than say the GTA. They also will take on more or less burden depending on the task at hand (regional containment of COVID19 being a prime and timely example). This goes for the subregions too – some sections might turn on more or less depending on the degree of arm elevation, your plane of movement, and resistance.
If that’s the case, then is there a way to make rehab more specific by targeting movements that bias one subregion over another?
I was hoping the answer would be yes, but the research isn’t there yet. It seems as though there are still some discrepancies in the research about which subregion does what. Furthermore, the role of the inferior infraspinatus has yet to be determined.
I have summed up 4 key takeaways below in terms of the roles of the subregions:
All three subregions of infraspinatus are more active the higher your arm is in front of you (eg: they will work harder if you are reaching into a high cupboard, and will work less if reaching for something at waist height).
The superior infraspinatus has a shared insertion on the top of the arm bone with your supraspinatus (another RC muscle that will have its own blog post next). It is thought that both muscles contribute to shoulder stabilization, and that redundancy allows for people to have tears and still be strong.
The middle infraspinatus is more of a pure external rotator.
There is minimal evidence for the role of the inferior infraspinatus.
What does this mean for rehab?
When you are dealing with a fresh injury, start with exercises where your arm is low and closer to your body, like farmer’s carries. Any load on your arms will turn on your rotator cuff, and this is the least provoking position to be in.
You can start with isometrics (exercises where you are not moving your arm through range) if you cannot even move the shoulder without pain.
You don’t have to rotate your shoulder to get your infraspinatus. You can just do an arm raise and it will work all three subregions. The higher your arm, the more the infraspinatus will be working.
Generally, strengthening external rotation follows the same principle. The movement of rotating your arm outward will be more challenging the further away your upper arm is from your body (overhead vs tucked into your side).
Check out the video below for 4 different exercises that target the infraspinatus, ranging from lower muscle activation to the most, using the principles I outlined above. Some of these exercises are based on articles published by researchers at the Digital Industrial Ergonomics and Shoulder Evaluation Laboratory at the University of Waterloo (local shout out!).
The next write up will target the supraspinatus – yet another notorious RC muscle that also has 2 subregions despite being super slender. As I eluded to above, superior infraspinatus shares an insertion with supraspinatus, and we will talk about why that is so important for shoulder stability and how you could approach rehabilitation for a torn supraspinatus. Stay tuned!
Sayaka is an evidence based physiotherapist in Waterloo. Click here